
The Invisible Made Visible
How a quiet government survey revealed the chemical reality of everyday life—and the power of prevention


Measuring a Nation, One Person at a Time
It doesn’t look like a laboratory.
The trailer is parked in a school lot, its steps worn from years of use. Inside, the air is cool and clinical. A nurse draws blood while another technician calibrates a machine that will measure something most people have never heard of—and never asked about. Outside, a line forms: a truck driver, a grandmother, a teenager who was told to skip breakfast.
They are not patients. They are participants.
Each will leave with little more than a thank you. But together, they are building something far more valuable: a portrait of a nation’s health, drawn not from clinics or hospitals, but from everyday life.
For more than half a century, the National Health and Nutrition Examination Survey—NHANES—has done something no clinic, hospital, or randomized trial could do. It has measured us as a population: what we eat, what we carry in our blood, what is changing—and what is not.
It has, in a very real sense, made the invisible visible. And yet, for all its influence, NHANES remains largely unknown outside public health.
The Decision to See Clearly
The effort to measure the health of Americans began with a quiet but consequential piece of legislation. The National Health Survey Act of 1956 authorized a continuing, nationwide survey to measure the amount, distribution, and effects of illness and disability. It marked a shift in how government approached health—not simply treating disease but measuring it across the population.
That shift was driven, in part, by a changing pattern of disease. Infectious diseases were receding, while chronic conditions—heart disease, cancer, and stroke—were emerging as the leading causes of death and disability. These were not diseases that appeared suddenly or spread through outbreaks. They developed slowly, often invisibly, and were shaped by the conditions of everyday life.
The mandate led to the National Health Interview Survey in 1957 and, soon after, to the National Health Examination Survey, which added direct physical exams. Instead of relying on hospital records or physician reports, federal officials chose to collect data directly from households and communities. Blood pressure was measured. Vision and hearing were tested. Children were examined for growth and development.
This was not glamorous work. It was logistical, methodical, and expensive. But it reflected a new idea: understanding health required seeing it where people lived.
Still, these early surveys could describe illness better than they could explain it. They could tell you who was sick, but not why.
Connecting Behavior, Biology, and Disease
That gap led to a second decision. In 1971, federal health officials expanded the survey to include nutrition, launching NHANES. This was more than a change in name. It was a change in purpose.
Now, the survey could connect behavior, biology, and disease. It could link what people ate to what appeared in their blood and how their bodies functioned. It could begin to trace the pathways between exposure and outcome.
Subsequent phases built on that foundation, including NHANES II, which began in February 1976 and continued through 1980, and NHANES III, which expanded the scale and scope of measurement even further. By the time NHANES III was completed, the survey had matured into a national instrument—capable not just of describing health, but of helping to explain it.
With each iteration, the survey moved closer to its central aim: not just to document disease, but to understand how it arises—and how it might be prevented.
When Exposure Became Visible
One of the most consequential decisions within NHANES was to include a blood test for lead. At the time, lead poisoning was still framed as a problem of extremes—industrial exposure, peeling paint, severe cases. If exposure was not obvious, it was assumed not to matter.
That assumption began to shift in the mid-1970s. As NHANES II (1976–1980) was being planned, concern about low-level exposure was growing.
The push to measure blood lead came through an interagency effort, but one figure was pivotal. Kathryn Mahaffey, then at the FDA, recognized the need for nationally representative data and helped ensure that blood lead testing was included.
NHANES operates on a simple principle: agencies that want specific measures added must help fund them. With support from FDA and others, the resources were secured. Once in place, the proposal fit squarely within NHANES’ mission, and there appears to have been little resistance at NCHS.
What followed was a revelation.
When blood lead levels were measured across the population, it became clear that exposure was not rare. It was widespread. Children across the United States—regardless of geography—had measurable levels of lead in their blood. What had been considered a niche problem was, in fact, a population-wide exposure.
Then something even more important happened. As policies were implemented to remove lead from gasoline, NHANES tracked the results. Blood lead levels fell—dramatically and consistently—across the entire population.
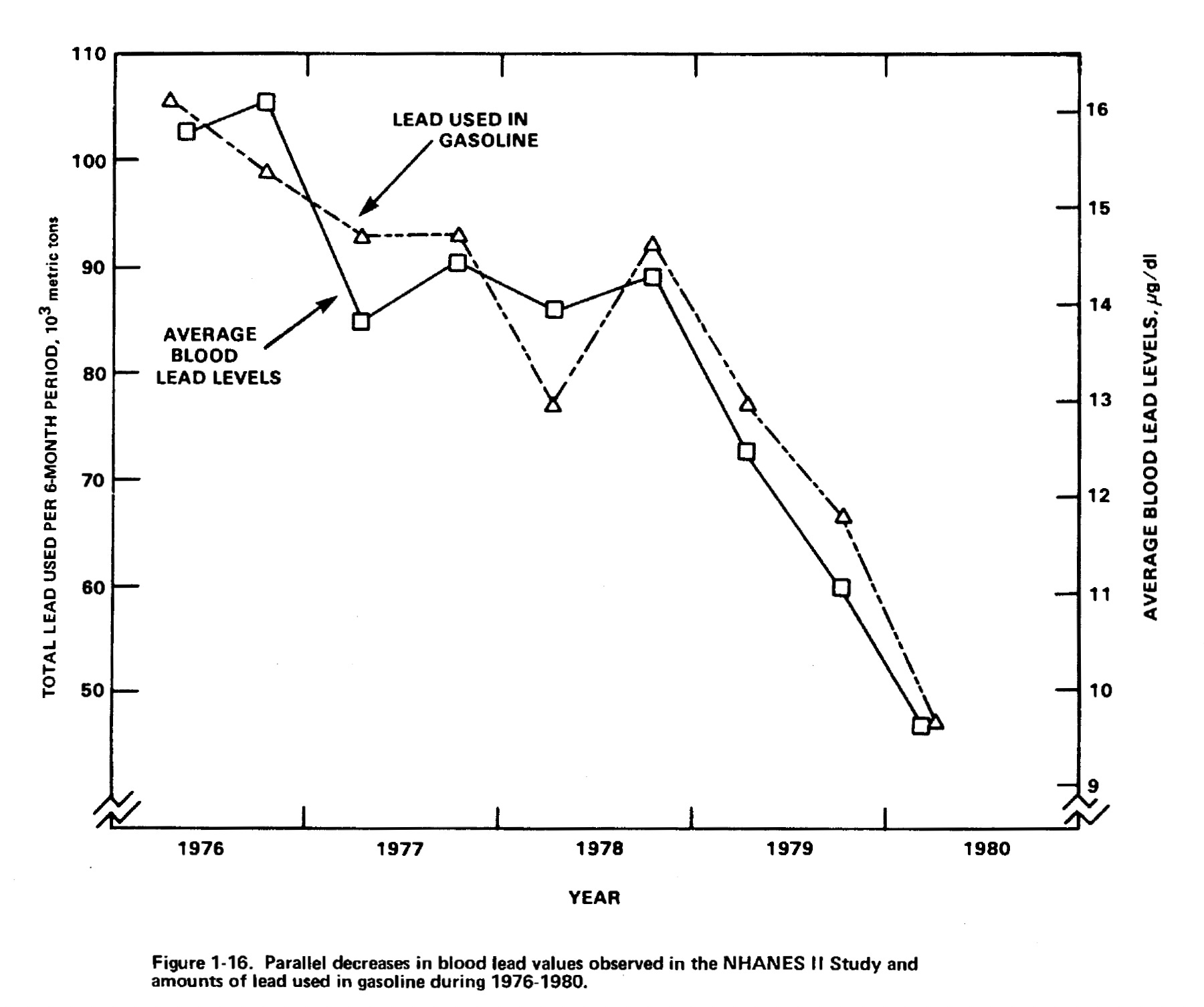
This was one of the clearest demonstrations in modern public health that reducing exposure can shift the health of a nation. It did not depend on treatment. It depended on prevention.
NHANES did not create that policy. But it made its impact undeniable.
From Snapshots to Surveillance
For decades, NHANES operated in cycles. Data were collected, analyzed, and then the survey paused before the next phase began. That model produced important insights, but it limited the ability to track change over time.
In 1999, federal officials made another pivotal decision: NHANES would become continuous.
Each year, mobile examination caravans would visit communities across the United States, collecting data from a nationally representative sample. This transformed NHANES from a series of snapshots into a moving picture. Trends could now be observed as they unfolded, rather than reconstructed after the fact.
This was surveillance in the best sense of the word—not monitoring individuals, but understanding patterns across a population.
Linking Exposure to Outcome
Another innovation extended the reach of NHANES beyond measurement: mortality follow-up. By linking participants to national death records, government scientists created a bridge between exposure and outcome. Measurements taken at one point in time could now be connected to events years or decades later.
This transformed NHANES into something more than descriptive. It became explanatory.
Researchers could examine how blood pressure predicts mortality, how diabetes shortens life, and how physical activity influences long-term risk. It also made it possible to examine environmental exposures in a new way.
NHANES, with its nationally representative biomonitoring and mortality follow-up, provided some of the first rigorous evidence that low-to-moderate levels of metals like lead and cadmium—well below existing thresholds—were linked to cardiovascular disease and death. It helped move these exposures from the margins into mainstream cardiovascular risk assessment, on par with traditional risk factors. In my own research, we linked blood lead levels to mortality and found that lead exposure was the leading risk factor for coronary heart disease deaths—surpassing even smoking.
What had once been considered a narrow toxicological concern emerged as a major population-level risk factor. NHANES made that connection possible—not through a single experiment, but through sustained measurement over time.
From a Few Chemical to Hundreds
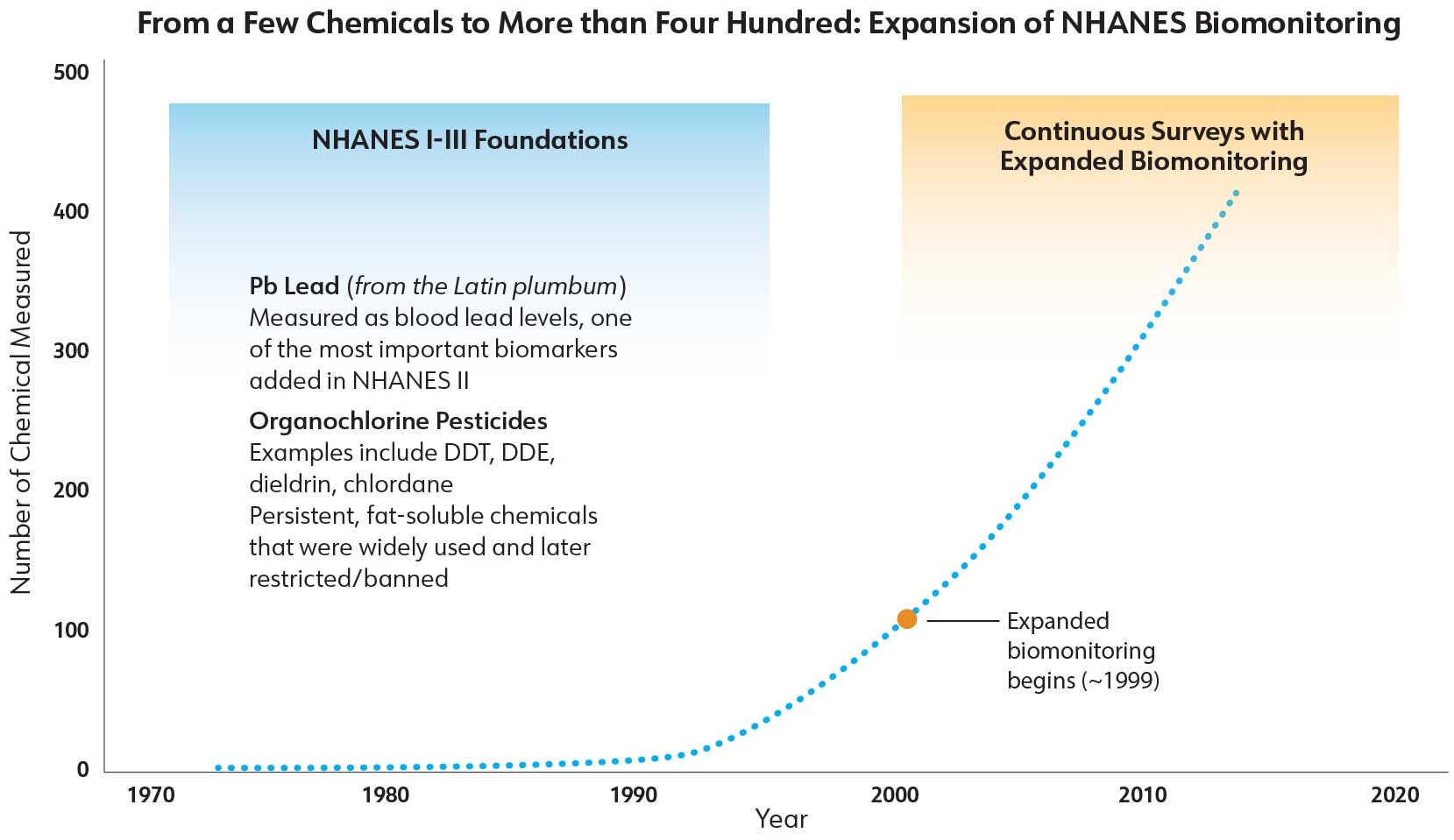
Over time, the scope of NHANES expanded beyond a few key biomarkers to include hundreds of chemicals. This evolution reflected another shift in thinking within government: that exposure should not be inferred indirectly when it could be measured directly.
When NHANES began in the 1970s, it measured only a few environmental chemicals—most notably blood lead and organochlorine pesticides, like DDT. It was a narrow but important window into exposure at a time when leaded gasoline and legacy pesticides dominated concern.
Today, NHANES measures more than 400 hundred chemicals in blood and urine, including metals, pesticides, plasticizers, flame retardants, and per- and polyfluoroalkyl substances. We have moved from tracking a few well-known toxicants to surveying a far more complex chemical landscape—one that includes mixtures, short-lived compounds, and emerging contaminants, many of which remain poorly understood.
This approach—biomonitoring—asked a simple question: what is actually inside the human body?
The answer was remarkably consistent. People were not exposed to one chemical at a time. They were exposed to many, often simultaneously, at levels low enough to escape clinical detection but high enough to raise questions about long-term effects.
This was not the model that risk assessment had been built on. Traditional approaches assumed discrete exposures and clear thresholds. NHANES revealed a more complex reality: continuous, cumulative exposure across the population.
Living in a Chemical World
NHANES helped normalize a new understanding of risk. The older model assumed identifiable hazards and clear lines between exposed and unexposed groups. The new model was less comfortable.
Exposure was widespread. It was ongoing. And it was layered. We were not living in a world of isolated risks. We were living in a chemical world.
This did not mean that every chemical caused harm. But it did mean that the burden of exposure was shared, and that understanding its effects required new ways of thinking—about mixtures, timing, and cumulative impact.
From National Tool to Global Standard—With a Critical Blind Spot
The success of NHANES did not go unnoticed. A few countries built similar systems, adapting the model to their own populations. Canada established the Canadian Health Measures Survey, or CHMS. South Korea launched KNHANES.
Each reflected the same insight: that understanding health requires direct, population-based measurement—not just of disease, but of the conditions that produce it.
But the deeper lesson has been only partially learned. Most countries still do not measure industrial chemicals in their populations in any systematic way. That absence is not a technical limitation—it is a failure of public health surveillance.
In the 21st century, where toxic metals and synthetic chemicals permeate air, water, food, and our bodies, biomonitoring is not optional. It is foundational. Without it, we are left to track disease while ignoring its upstream drivers—measuring the consequences while remaining blind to the causes.
A Quiet Engine of Evidence
NHANES has been used in more than 30 thousand publications. Its data underpin clinical guidelines, environmental regulations, and public health recommendations. It informs how we define normal, how we detect risk, and how we measure change.
And yet, NHANES itself rarely appears in headlines. It does not produce a single discovery. It produces a steady accumulation of evidence.
It is infrastructure for knowledge—quiet, persistent, and essential.
The Next Questions
For all its strengths, NHANES has limits. It measures individuals at a point in time, which makes it difficult to capture trajectories. It measures chemicals individually, even though real-world exposure occurs in mixtures. It provides biomarkers, but not always the biological pathways that connect them to disease.
These limitations matter because the questions we now face are more complex. What is the combined effect of multiple endocrine disruptors? How do environmental exposures interact with genetic susceptibility? Why are some chronic conditions rising so rapidly that we struggle even to track them?
These are not peripheral questions. They are central to understanding modern disease.
Toward a More Complete Picture
The solution is not to abandon NHANES, but to build on it. A larger and more integrated system could begin to address these gaps. Expanding the sample size would improve the ability to study less common outcomes and vulnerable subgroups. More systematic integration of genomic and emerging epigenetic data—building on existing NHANES biospecimens—would strengthen the study of gene–environment interactions. And improving the assessment of cumulative and repeated exposures would better reflect real-world conditions.
Following individuals over time would transform the survey from a series of measurements into a narrative of health across the life course.
Such a system would require investment. It would also require a shift in priorities—from reacting to disease to anticipating it.
The Pattern Beneath Disease
NHANES did something deceptively simple. It measured the population. But in doing so, it changed how we think about disease.
It showed that disease is not random. It is shaped by environment. And, in many cases, it is preventable.
Because NHANES is representative of the population, it allows us to go a step further—to calculate how much disease, and how many deaths, can be attributed to specific exposures. These calculations translate risk into consequence. They move us from association to accountability.
And once you can attribute disease to an exposure, the question is no longer whether it matters. It is whether we are willing to act.
Seeing Clearly Is Only the Beginning
We have built a system that can see what was once invisible. We have measured exposures, tracked their decline, and linked them to health outcomes. We have shown that prevention is not only possible, but powerful.
And yet, we hesitate. We debate, we delay, and we ask for more certainty—even when the pattern is already clear.
NHANES is still operating, but not as securely as it once did. After being suspended during the pandemic, it was relaunched in 2025. The trailers keep moving, the blood keeps being drawn, and the data continue to accumulate—quietly, patiently—waiting for us to catch up. Yet the system that once measured a nation with steady precision now shows signs of strain: fewer participants, disrupted cycles, and the growing challenge of maintaining a truly representative sample.
That tension—between what we can see and what we are willing to do about it—points to something deeper. Once you measure a nation, you inherit a responsibility: not just to observe, but to act; not just to describe what is happening, but to ask why and to change it. We built a system to see ourselves clearly. What we do with that vision is no longer a scientific question—it is a moral one.
What we measure is not just a technical decision—it determines what becomes visible. And what remains unseen can shape our understanding of health for years, even decades.
Great read! Is NHANES at any risk under the present anti-science administration. It seems to me to be right up MAHA’s alley, measuring hard data as affected by lifestyle. Where does NHANES get its funding from? I think it should be ramped up. I was struck by the graph on lead levels. In the 1970’s was it really that high? I’m 81 yo and, as a child, played with lead toy soldiers…I was probably in the hundreds! Never having been chelated, does the risk remain with me many years later?
My head is reeling and spinning......so much data.....so much information.....so many interactions........Thank you for trying to get us all to understand the complexity and the necessity and the urgency........it will take me many readings to get it all compacted into my brain into a useful simplicity of understanding. I am with you Bruce, just a little slow at wrapping my head around it all......